The Cognitive Invalidation Approach to Panic Disorders
Malcolm McFadyen
Chapter 13, Panic Disorder: Theory Research and Therapy, Edited by Roger Baker (c) 1989 John Wiley & Sons
In seeking to understand and treat a disorder the clinician draws on two sets of related formulations. The first is about the nature of the disorder – what is “wrong” with the person, and how the condition, state or syndrome has developed. The second is about the nature of the process, or processes, whereby one’s therapeutic interventions are considered to have their effect – how does the treatment work?
These formulations are influenced by many factors – training, reading, clinical experience and assessment of research evidence. This is an ongoing process. No formulation can be claimed as proven. Aspects can be consistent or not consistent with research results, and when inconsistencies are established one has to modify the model accordingly. Likewise, new “insights” based on clinical experience generate the need for further research to test validity. At any one time, the clinician operates on the basis of his “best informed” formulation. This chapter presents a clinician’s best informed formulation of panic disorder, and of its treatment by the behavioural technique of prolonged in vivo exposure.
It takes as a starting point the evidence of the effectiveness of behavioural exposure techniques (Marks, 1978a) in agoraphobia. Paradoxically, as the evidence for the effectiveness of these techniques grows, there has been increasing dissatisfaction with the conditioning models on which the techniques were based, both the model of the nature of agoraphobia and the model of how prolonged exposure works (Baker and McFadyen, 1985; Hallam, 1978; Marks, 1978b). It is not my purpose here to present a detailed examination of the inadequacies of these models, but the main points of complaint have been the model of agoraphobia as a conditioned avoidance of public places is not consistent with known clinical features, and that while conditioning theory gave the initial impetus for the development of behavioural approaches, it has failed to continue to provide direction to research into, or development of, behavioural techniques.
The most significant change in thinking about the nature of agoraphobia has been a move away from considering it as being essentially like the common phobias such as snakes or spiders, with the difference being only in the object of fear. There is now evidence that the differences between agoraphobia and the other more common phobias are more important than the apparent similarities. They have different clinical features (Klein, 1981; Snaith, 1968; Hallam, 1978, 1985), and a quite different etiology (Agras et al, 1969, 1972). Hallam (1978) has convincingly argued that agoraphobia has more in common with other anxiety states of the kind usually now referred to as panic disorder.
We are thus left with an effective technique with a less than satisfactory rationale, applied to a disorder about which our thinking is undergoing radical change. It is against this background that many are seeking new formulations. The particular approach described here is one such attempt developed from the standpoint of a practising clinician. It is hoped that the ideas offered hold promise both of an increased theoretical understanding of the panic disorders, and of improving and extending the applicability of behavioural exposure.
A GENERAL MODEL OF ANXIETY
Before describing the formulation of panic disorder, it may be useful to briefly consider how normal anxiety is viewed. It has been pointed out by Epstein (1972) that the conditioning view of anxiety as simply an aversive state analogous to pain is a minority view. Many theorists on anxiety (Spielberger, R.S. Lazarus, Liddel, Goldstein, Rogers, Mandler, Kelly) emphasize the central role of cognition. The model represented schematically in Figure 13.1 is derived from the work of Speilberger (1966, 1972), Lazarus and Averill (1972), Lazarus and Lannier (1978) and Kelly (1955, 1963). Spielberger and Lazarus present similar positions. The central postulate of both is that anxiety is generated and maintained by a person’s “appraisal” of threat. Both writers include physical and psychological harm (or potential harm) in their concept of threat. Lazarus distinguishes different aspects of appraisal: “primary” appraisal referring to estimation of potential harm; “secondary” appraisal referring to estimation of our capability to cope with the threatened harm, and “reappraisal” based on feedback – this latter characterizing appraisal as a dynamic rather than static process – over time we continue to reassess the danger and our ability to cope.
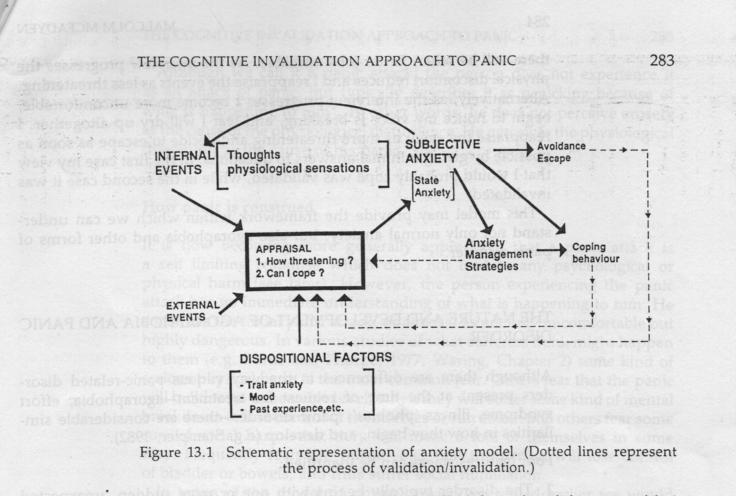
Kelly’s concept of validation/invalidation is added to provide the process through which our appraisal is continually modified by experience. Kelly states, “Validation represents the compatibility (subjectively construed) between one’s prediction and the outcome he observes. Invalidation represents incompatibility (subjectively construed) between one’s predictions and the outcome he observes” (Kelly, 1963 p.158).
The model states that threat may arise from external or internal events, or some combination of these – e.g. a job interview (external event); chest pain (internal event); an examination which we fear we will fail (combination of external and internal events). If I appraise the event as threatening and am uncertain of my ability to cope I experience subjective anxiety, which may consist of either, or both, of thoughts (say, fear of possible negative outcome) and of physiological sensations (nausea, tremulousness, etc.). The loop with internal events indicates that these add to the external events being appraised. At this point I may opt to avoid or escape the situation, or I may opt to attempt to cope with the event, depending on my judgement of likely outcome. I may use anxiety management strategies to help me cope – deep breathing/relaxation, reasoning thoughts. At any of these stages my experience may confirm my appraisal or contradict it. Suppose I am in a difficult job interview and am feeling nauseous and tremulous, I think I can probably cope if I keep these under reasonable control through practising relaxation, or reassuring myself that anyway, there will be other, better jobs available. As the interview progresses the physical discomfort reduces and I reappraise the events as less threatening. Alternatively, as the interview progresses I become more uncomfortable, begin to notice my voice is breaking, and fear I will dry up altogether. I reappraise the event as more threatening and decide to escape as soon as possible by giving minimal answers to questions. In the first case my view that I would probably cope was validated, while in the second case it was invalidated.
This model may provide the framework within which we can understand not only normal anxiety, but also agoraphobia and other forms of panic disorder.
THE NATURE AND DEVELOPMENT OF AGORAPHOBIA AND PANIC DISORDER
Although there are differences in the way various panic-related disorders present at the time of request for treatment – agoraphobia, effort syndrome, illness “phobias”, panic disorder – there are considerable similarities in how they begin, and develop (e.g. Stampler, 1982).
Four features can be identified:
1. The disorder typically begins with one or more sudden, unexpected full-blown panic attack.
2. These events are construed as highly dangerous.
3. Following the early spontaneous attacks the person becomes afraid of, and therefore oversensitive to internal physiological sensations.
4. The sufferer develops strategies to avoid, escape or minimize the feared effects of panic attacks.
The first panic attack
These attacks are qualitatively different to high anxiety (Freedman et al, 1985). The body responds as if you had a severe fright, but in the absence of any obvious precipitant. The symptoms consist of varying combinations of palpitations, tachycardia, shortness of breath, dizziness, nausea, tremulousness or weakness of limbs, and sweating. The event is experienced as highly physical and highly aversive.
Although we call it a panic attack, the person does not experience it as an attack of panic, but typically describes it as panicking because of what is happening to him*. In other words, he does not perceive anxiety as the cause of the physiological disturbance. He perceives the physiological discomfort as the cause of his panic.
How panic is construed
It is now becoming more generally appreciated that a panic attack is a self limiting response which does not lead to any psychological or physical harm (see later). However the person experiencing the panic attack has no immediate understanding of what is happening to him. He construes the initial panic attack, or attacks, as not only uncomfortable but highly dangerous. In various studies of what sufferers think might happen to them (e.g. Burns and Thorpe, 1977; Waring, Chapter 2) some kind of serious physical harm is the most common fear. Others fear that the panic will build to an unbearable level, when they will suffer some kind of mental breakdown or lose control of themselves or run amok. Still others fear some sort of social harm – that they will make a fool of themselves in some way. Frequently fear are mixed – e.g. that the person will lose control of bladder or bowels, and thus suffer social humiliation.
In terms of the model of normal anxiety presented earlier we would suggest that the extreme fear reported in panic attacks is not simply due to the unpleasant nature of the physiological disturbance, but is mainly due to the interpretation of these as physically or psychologically dangerous. In other words, the extreme anxiety is understandable in terms of the person’s appraisal of what is happening to him.
There is some evidence of the role of interpretation, or appraisal, in the responses of subjects in the study by Pitts and McLure (1967) who showed that subjects who had an anxiety disorder tended to report a panic attack when infused with sodium lactate, whereas “normal” subjects did not. Pitts and McLure quote one “normal” subject as saying “If I didn’t know you were doing this to me, and that you wouldn’t let anything bad happen to me, I would be certain I was dying of a heart attack or something terrible”.
The catastrophic appraisals of panic attacks need not be regarded as irrational, or illogical or “distorted”, as suggested, for example, by Beck and his colleagues (1985). We do not know that panic attacks are not harmful through reason or logic, but through experience. It is suggested that such an interpretation is not distorted, but may be a common response to the experience of a panic attack.
The particular form of catastrophic thinking will vary from sufferer to sufferer. Some may focus on the particular physical symptoms and worry about having a heart attack, a brain tumour or stroke. Such variations are likely to be influenced by differences in past experiences. For example, sufferers with family experience of mental illness may tend to interpret the threat as psychological.
Development of over-sensitivity to autonomic change
Following the early, unexpected, panic attacks the person usually, and perhaps not surprisingly, becomes afraid of sensations related to change in autonomic activity, with a consequent over-awareness, and over-monitoring, of internal physiological sensations. This development has the effect that later panic attacks are frequently self-induced. The person is alert for any sign of threat from within, leading him to be over-aware of normal symptoms of autonomic change which he now perceives as a potential threat – the start of another attack – thus setting off the body’s natural fright response. Such a process is implied in the frequently used phrase to describe this stage of development as “fear of fear”. From a different theoretical perspective this has been described as “interoceptive conditioning” (Goldstein and Chambless, 1978).
Thus the early, unexpected, panic attacks can often be distinguished from the later ones which are set off through this fear of fear, or fear of having a panic. Perhaps we should restrict the term panic attack to the early, unexpected attacks, with a term such as panic reaction to describe the later self-generated responses.
The development of strategies to avoid, escape, or minimize the effects of panic attacks
After one or more panic attacks it is not surprising that the person develops various strategies to avoid, escape, or minimize the feared harm. This can mean avoiding certain activities – physical exertion, or avoiding certain situations – shops, public transport, crowds (the agoraphobic triad), or it may mean a more pervasive avoidance of potentially upsetting events.
Where avoidance is not always seen as possible or necessary, many sufferers take steps to have an escape route available. This could be literal in the sense of being near an exit, or metaphorical in having a prepared excuse for leaving a situation.
Finally where avoidance or escape are impossible or impractical, sufferers attempt to minimize the anticipated effect of a panic attacks. The person who fears a heart attack may cease activity. The person who fears that he will be unable to sit still, or who fears that others will see him shaking or sweating, may engage in some activity to minimize this risk.
These strategies will not only involve defining what the danger is, and what must be avoided, escaped or minimized, but will also involve identifying “safety” factors (Burns and Thorpe, 1977) – conditions which the person thinks will act to reduce the perceived risk, such as being with a friend, taking alcohol or tranquillisers.
All of these strategies are designed to prevent the outcome which the person fears will result if a panic attack were allowed to occur or to continue unchecked, and they therefore effectively prevent the person from discovering that the harm he fears does not happen.
THE SELF-MAINTAINING NATURE OF PANIC DISORDER
The features of agoraphobia and other panic disorders may be readily understood in terms of the general model of anxiety presented earlier.
Once the person misconstrues the nature and consequences of his panic attacks the other features are natural and normal developments. Over-sensitivity to autonomic symptoms results in the threat being continued beyond the original unanticipated panic attacks, and avoidance/escape/minimizing strategies effectively serve to prevent correction, or invalidation, of the interpretation of panic as dangerous. At this stage the disorder is effectively self-maintaining.
WHAT CAUSES THE FIRST PANIC?
Up to now we have been concerned with the development of panic disorder/agoraphobia after the early “spontaneous” panic attacks. How are these first attacks accounted for?
It is suggested that there is no need to postulate a physiological (e.g. Klein et al, 1985; Sheehan, 1982) or psychological (Goldstein and Chambless, 1978) abnormality as a necessary condition for these first panic attacks. It has already been suggested that the bodily reactions described by patients can be regarded as fright in the absence of any obvious external threat. It would seem reasonable to consider that there will be variations in the sensitivity of the trigger mechanisms of the body’s emergency response, and that at times of increased readiness to respond the system will occasionally trigger “spontaneously” – a kind of false alarm.
When a person is under stress, e.g. conflict at home or work, illness, bereavement, there is considered to be such an increase in the readiness to respond of the body’s emergency system – the so-called “fight or flight” response. Other factors will also cause an increase in readiness to respond – e.g. endocrinological variation such as hypoglycaemia.
A critical factor in determining the person’s reaction to such a false alarm would be whether he correctly construes the event. Evidence is lacking on the number of people who have such a reaction and correctly construe it. Misconstruing the event as unnatural and dangerous is certainly strikingly typical of patients, and perhaps of most people who experience this spontaneous triggering of the body’s fright reaction (see postscript).
The initial panic attack may be viewed as a normal, though not usual, stress reaction. There will obviously be many factors which affect a particular person’s vulnerability. Some people are typically more threat sensitive than others – Spielberger’s Trait Anxiety. However, such factors might better be seen as a predisposition to, rather than a prerequisite of, a panic attack.
DIFFERENCES IN HOW PANIC DISORDER PRESENTS
What determines that panic disorder in one person takes the form of agoraphobia, in another illness fears, and in yet another continuing unpredictable panic attacks? Some of this can simply be attributed to individual differences. Differences in interpretation of the symptoms will lead to differences in how the disorder develops. However, there is also the suggestion of change over time, with agoraphobia-type symptoms being more likely in later stages of development of panic-disorder (Klein, 1964). There will, of course, be other changes over time as the person continues to try to make sense of what is happening to him in the light of experience and information. Some people accept the view of their general practitioner, or other medical practitioner, that they are not physically ill, but are suffering from “anxiety”, but then construe themselves to be at risk of psychological harm – “loss of control”, “mental breakdown”, etc. For some people this change over time will mean a widening of what is regarded as potentially dangerous, for others it will mean a narrowing to only regarding certain specific conditions as threatening.
IMPLICATIONS FOR EXPOSURE TREATMENT
If the cause of the person’s anxiety is the harm that he anticipates could result if a panic attack continued unchecked, then any conditions of exposure which invalidate his expectation of harm will help to reduce his anxiety. At the simplest level he might discover through exposure that the panic attack which he expected does not occur. If the therapist has stressed some kind of anxiety management training he may come to believe that he has learned to prevent the panic attack.
The Cognitive Invalidation (CI) formulation suggests, however, that exposure will be most effective when the person puts himself in the feared situation under conditions of perceived risk – in other words, when the patient uses exposure to find out what does happen when he panics with no attempts at escape or control. If the person is panicking because he fears he will die, then finding that he does not must have a powerful anxiety reducing effect! This process is referred to as cognitive invalidation. The term “invalidation”, from George Kelly’s Personal Construct Theory, refers to the process whereby when outcome is perceived to be contrary to what we expect then we tend to alter our expectations.
EXPOSURE AS COGNITIVE INVALIDATION
Exposure can thus be considered as an experiment conducted by the patient in which he can test out his hypothesis that panic is dangerous and will cause him harm if he allows it to continue unchecked. As with any other experiment the experimenter has to have an understandable rationale for undertaking the experiment. Some time is therefore spent providing information about anxiety, explaining how it arises; how the body responds; how it is self-limited. And how it has no serious adverse after-effects. In particular, information would be provided on those sensations which most frighten the patient. For many, explaining their panic attacks as a false alarm fright reaction is sufficient for them to be able to comprehend how this could account for their panic reactions. Others wish to check through particular symptoms to seek reassurance that these are understandable in terms of the body’s emergency response.
Of course, by the time they present, many clients are experiencing over-sensitivity to physiological sensations and this also needs to be explained in order that they can make sense of their experiences. Many symptoms are better understood as over-sensitivity rather than the fright reaction – for example, the more pervasive feeling of physiological discomfort complained of by many patients.
Having provided this alternative explanation of their experiences, it is often unnecessary to propose exposure. Simply asking what the person needs to do to be convinced that they will not come to harm usually leads them to suggest the need for exposure. Further discussion may be needed to help the person tighten the design of his “experiment”. This aims for an exposure session during which the person commits himself to having a panic attack without attempts at control, avoidance or escape.
At this stage the therapist’s role is akin to that of research supervisor, an analogy previously suggested by Kelly (1970). However, it differs in one important respect – the research supervisor is rarely in the position of advising a student on an experiment on himself which the student regards as potentially dangerous. The design of the initial experiment will be less than perfect – it will be limited by the degree of risk the person is prepared to take. This usually results in a starting point for exposure which is not the worst situation the person fears, but is still one which carries significant risk – in effect, a steeply graded exposure programme. At this stage we cannot plan the complete series of experiments which will be necessary. As with any other research programme, later experiments will best be planned to take account of the results of earlier experiments.
Let us assume the person has gone off and completed the first ‘experiment’. He has had a panic and has not attempted to escape or minimize its effect. The panic, although acutely uncomfortable, has indeed passed without him having come to whatever harm he feared. Should he now accept the alternative hypothesis – that his panic is a normal, non-harmful, self-limiting response? As with any researcher where the result is not as expected, he is sceptical. A number of “replications” might be expected before the results are considered reliable.
Not only could one expect repetition, but it might be expected that the person will vary conditions, to be satisfied that the results are not limited to only certain circumstances. It might also be expected that the person will increase the level of “risk”. With each exposure the person’s prediction of a harmful outcome is invalidated until the prediction is no longer considered tenable – at which point “treatment” is complete.
This account shows such exposure to be a more individual programme rather than a fixed “package”. The patient is in control, and it is his reappraisals after each exposure (“reconstructions” in the language of Kelly’s Personal Construct Theory) which guide the programme. Therapy is a joint venture with both the therapist and the patient having clear but different responsibilities. The therapist’s responsibility is to help the patient understand what he is doing and why. The patient has final responsibility for the “experiments” and the conclusions drawn. Some examples will help to illustrate the process.
COGNITIVE INVALIDATION WITH AN AGORAPHOBIC PATIENT
Mrs X was in her early thirties, married 13 years to a tradesman painter, with 3 childen between 6 and 12 years. Her symptoms began about five years previously with a sudden attack of “giddiness”, palpitations and shortness of breath while she was waiting for a bus at a stop near her home. She initially interpreted the symptoms as having a physical origin. She had gone to a neighbour’s house close to the bus stop – “I thought I would never make it”. Husband was summoned to take her home, where she went to bed. The family doctor was called and after a brief physical examination he pronounced her physically well and told her that her symptoms were “anxiety”. Further panic attacks occurred over the next two months, one while queueing at the check-out of a supermarket, and one waiting to have her hair done. Over this time, Mrs X increasingly began to avoid situations involving shopping, travelling by public transport and other situations where she felt “restricted” – restaurants, theatre, church. The latter particularly concerned her as both she and her husband were very much involved in church activities. After the first few panics she had begun to anticipate them and often abandoned planned outings. Further trips to her GP led her to understand that she had agoraphobia and she was prescribed a common benzodiazepine.
By the time of presentation she accepted that she was not physically ill, but feared that she would be overcome by the panic – that she would pass out or make a fool of herself. Life had been adjusted to fit with her disorder – she could go most places if accompanied by her husband, or her 12-year-old daughter, but she avoided completely church, theatre and restaurants. On “good” days she could do some shopping on her own, as long as she avoided long queues. On “bad” days she would stay at home. She avoided planning outings, or committing herself to outings in advance. She preferred to wait to see how she felt. Her confidence generally was poor – “I was never a particularly confident person, but not like this”. She used a benzodiazepine drug intermittently to help her cope with necessary outings, particularly on “bad” days. Her understanding of her disorder was still rather vague, but was mainly construed as the psychological equivalent of having a “weak heart” – she would be all alright as long as she did not allow herself to get “too upset”.
Over the first two appointments, one week apart, she was given the explanation that her panics could be seen as a kind of false alarm of the body’s fright response; how panic attacks could relate to stress. The subsequent development of over-sensitivity to physiological sensations was also explained.
These accounts “made sense” to her, and she expressed relief that her symptoms might be understandable as a normal reaction. She was able to provide a number of possible “causes” for her initial panic attacks – she had been worrying about her mother who had been seriously ill prior to the onset of her symptoms. She had been feeling fed-up being at home for some time, but the last child prevented her return to work. There was some guilt associated with these feelings and she felt unable to talk to anyone about this for fear of being considered a bad mother.
The “over-sensitivity” made sense of her “good” and “bad” days. She was able to talk about how she tried to avoid potential upsets as this tended to result in “bad” days.
Although she considered that the explanation made sense of her experience, and quickly appreciated how she could only confirm this by allowing herself to panic, she was very unsure as to whether she could take the necessary risks. After some discussion she proposed a trip to a supermarket as a first target, and set a goal of at least two such trips without the help of drugs before the next appointment in two weeks time.
At the next session she reported having gone on three such trips, with her husband who had waited outside in the car. She had briefed him on the nature of her “experiment”. This had been “hell” – she panicked almost continuously and had been on the point of leaving two or three times. However, she had waited and the panic did pass, after about 45 minutes, without her passing out or making a fool of herself. She admitted that she had not gone through the check-out until after the panic had subsided. She had felt exhausted but pleased with her first session.
The second trip was “even better” – she had expected to panic, but it did not happen. The third was “a disaster” – she had a major panic attack which did not stop until she left the shop. It left her feeling bad for days.
We discussed the interpretations of the “outcomes” of her “experiments”. She was asked in what way was the second trip “better”? How did it affect her confidence that she would not pass out if she did panic in future? She was able to acknowledge that in fact she had really learnt nothing from this trip. She had been so pleased that no panic had occurred, that she re-set her objectives – i.e. she hoped she would not have another panic. This was why the third trip was very informative – she had not passed out – she had not made a fool of herself – and she had gone through the check-out! She had come in looking rather downcast, and left looking much brighter, with a commitment to adding a cinema trip to her two supermarket trips.
At the next session two weeks later, she reported having a panic attack only once in three trips to supermarkets (she went to two different ones). While she was pleased with the times she did not have a panic, she no longer regarded them as opportunities to “experiment”. The time when she did panic again produced a negative outcome in terms of passing out, etc. She had gone to the cinema with her husband – could not say she enjoyed the film – indeed at times had hardly been able to concentrate because she was so scared by the panic attack she was having. However, again she was pleased. She had not passed out, nor made a fool of herself. Why she chose a cinema rather than a theatre was because “it is darker – no one can see you properly”. She admitted she had gone when it was relatively quiet and had occupied an aisle seat.
Two weeks later she was reporting having been to church. Again she had been very uncomfortable because of a panic attack, but she had not passed out, and had not felt foolish in spite of having considerable attention from people who were interested to see her back after such a time away. She had considered what she would say and was pleased that most people were highly supportive when she told them she was trying to overcome “agoraphobia”. By this time, supermarkets only rarely produced panic – usually when she was stuck in a queue. She admitted that on one occasion it had taken her by surprise and she had left the shop, but returned after she had “told” herself she should not miss the chance of another “experiment”. By this time she had also been into town by bus. Again on one occasion she admitted that she got off when a panic attack came on suddenly. On other occasions she had continued her journey in spite of a panic attack. She spontaneously reported having looked at her reflection in shop windows, and mirrors, during one or two panic attacks and was surprised that “you couldn’t see anything much on the outside”. This boosted her confidence.
Over the next few sessions she continued to set more difficult experiments and some of the early experiments became routine. She could travel on her own by car and bus, and shopping was “almost enjoyable”. She took the family to a pantomime – back of the stalls but not aisle seats – “I can’t remember much of the first half, but I actually enjoyed the second part – once I survived the interval with the lights up I knew I could survive anything”.
She took the occasional tablet – not during exposure “sessions” – during the early weeks, but voluntarily gave these up after six weeks.
In later sessions she was able to admit that her earliest exposure “experiments” had been on “good” days. She quickly realized this reduced their value, and thereafter deliberately went out to the supermarket on “bad” days. She commented that she could not have begun with exposure on a bad day – it would have been considered “too risky”.
We also discussed her loss of confidence more in later sessions using a non-directive counselling format. She was soon able to assert that she coped well with “real” problems – listing family illness, all the usual crises of bringing up a family, etc. She decided she no longer needed to “protect” herself. While she did not like being upset, she became able to accept that it was normal to have “bad days”, and no longer feared them, and her periods of upset or feeling “down” passed more quickly. She was also later able to acknowledge that a desire to return to work at some stage did not make her a “bad mother”.
Mrs X attended for 10 appointments, the first two at weekly intervals, then six at fortnightly intervals, one after a month and one after three months. At the final appointment she reported occasionally feeling “as if” a panic attack was going to occur, but it did not develop. She had had one “unexpected” attack during the meal at a dinner-dance. “I almost ran, but I remembered you had warned that it could happen. The meal was hardly enjoyable, and afterwards I had all the old feelings – I was sure I was not going to make it across the room – my legs felt like jelly. However, I forced myself, and as usual I made it. It stopped quickly after that, and I really enjoyed the dance. I expect it will happen again sometime, but I think I’ll be ready for it”.
By this time she did not avoid situations, and was enjoying going into town shopping. She still had days when things went badly and she was upset or “fed-up” but these were accepted as normal.
COGNITIVE INVALIDATION EXPOSURE WITH OTHER PANIC DISORDERS
Traditionally exposure has been seen as a treatment for agoraphobic disorders, with some form of habituation/extinction considered to be the process through which it worked (Marks, 1978b; Mathews et al, 1981). This is continued in the panic disorder literature where there is often the suggestion that some form of combined treatment is necessary – drugs for the panic attacks and behavioural exposure for the phobic avoidance (Klein, 1981).
If exposure is operating through invalidation of fear of harm, then it is readily extended to other forms of panic disorder. The simplest extension is where the condition for panic occurring is doing something rather than being somewhere. Here the person would be encouraged to engage in the avoided behaviour, e.g. physical exertion in the case of so-called “effort syndrome”.
A common variant of avoidance – either of places or activities – is an escape strategy. Here the person continues with life more normally, but is prepared to leave the situation or cease the activity at a particular level of perceived threat. For some, this will be onset of a panic attack. For others it will be at some level of discomfort which the person interprets as indicating likelihood of a panic attack. For these people, the necessary condition for invalidation is to be in the situation or engage in the activity without the usual escape.
What about the apparently more difficult situation, where the person reports his panics as entirely unpredictable, either in terms of place or behaviour? Here we can make use of two aspects of panic disorder.
One is the oversensitivity to normal fluctuations in autonomic activity. In the developed panic disorder the person is frequently hyper-alert to internal sensations as he construes these as potential signals of imminent panic. The person often reacts with the very panic response which he fears.
Alternatively one can use the fact that in the developed panic disorder the person usually develops some strategy for minimizing the construed threat of harm. Thus one person may stop whatever he is doing and sit down. Another, whose panics tend to occur when inactive, may engage in a distracting activity. Yet another may take a tranquilliser, or an alcoholic drink.
By encouraging the person not to engage in his usual strategy for minimizing the risk of whatever harm he anticipates, we can create the conditions necessary for him to invalidate his fear that panic will lead to harm. Often he can go beyond not engaging in a minimizing strategy, to maximize the risk by doing whatever he construes would be most dangerous.
For example, Mrs R. experienced most of her panics while at her place of work. She could not predict their onset, did not avoid attending work, but whenever she experienced a panic attack she would leave the factory building and go outside “for some air”. For her the condition necessary for invalidating her fear was to remain at her work station when a panic attack occurred. She quickly learned that she did not collapse and her panic attacks gradually reduced in frequency and eventually ceased.
Mr B. adopted a very active strategy towards dealing with his panic attacks – he ran. He used this both as a strategy for prevention, and a strategy for controlling the effects of a panic. He worked long hours, under pressure of time, carrying out complicated repairs to electronic equipment, and during the day he would experience “a build-up of tension”. He would often go for a run at lunchtime, and again in the evening to try to dispel this tension, and prevent it reaching “danger level”. Most of his always unanticipated panics which were not frequent would occur when he was trying to relax – watching TV, reading, etc. When this happened he would engage in activity – the more active the better. If he could not go for a run he would find something in the house to do. Apart from a short period in the early stages of his difficulty when he had taken propranolol, he had refused to consider other drugs. Although he no longer took the drug he carried it with him – “just in case”. He feared that if he allowed his symptoms to continue without such controls he would “crack up”, “have a mental breakdown”.
Mr B. was in his late twenties, and something of an adventurer. His leisure time had been divided between a number of dangerous sports at an international level which he wished to do again, should he ever “recover”. He was particularly demoralized by his panic disorder, having always considered himself “mentally very stable” – “the kind of person who did not have psychological problems”. The fact that he was experiencing these difficulties meant there was “a flaw” in him. He now regarded himself as a potential “liability”. At first he thought his panic attacks were due to physical cause and described himself as being “shattered” when all the tests proved negative and he was told he was suffering from “anxiety”.
He was very relieved when his symptoms were explained as a false alarm of the body’s emergency response and subsequent oversensitivity. He had some difficulty discussing potential sources of stress when his symptoms began about a year previously. He could comprehend physical threat, but admitted he had no concept of other kinds of stress. He indicated he would prefer to try to deal with his difficulties at the symptom level, and only if necessary would he wish to explore potential sources of stress.
He quickly grasped the concepts and implications of the cognitive invalidation approach, and threw himself into an exposure programme with his usual energy. This involved allowing the tension to build up without running or other activities aimed at dissipating the tension. When he had a panic attack he was to sit quietly without attempts at distraction until it passed. He voluntarily disposed of his last few propranolol tablets.
Most of the therapist input was directed to supporting him through the few times when he “flunked” an “experiment” – that is, when he engaged in activity before waiting to see if he “cracked up”. Some time was spent allowing him to examine and challenge his view that “real men don’t flunk it”. He was able to do this quite successfully and with some humour at his “a man’s gotta do what a man’s gotta do” approach to life, which he had not fully appreciated before.
After six sessions over 3 months he declared himself symptom free. He was still aware of tension at times, but no longer worried about it. Further panic attacks were seen as quite possible, but manageable. Interestingly he thought he would now be more understanding of people with psychological problems, whom he had previously considered “just neurotic”. He hinted that he had “a good idea” how the panic attacks had begun, but felt he did not need to discuss this. He had resumed his high risk sports activities and was pleased that he had not proved a “liability”.
These examples give some indication of how the cognitive invalidation approach to panic disorder is put into practice. Both the longer examples are chosen to represent recurrent themes in therapy sessions which are seen as helping the person understand what is happening to him in such a way that he can use this understanding to deal with the problem actively and constructively. Part of this process may involve counselling towards helping the person appreciate and, if appropriate, resolve the source of the initial stress. The central focus, however, is on encouraging the person to test, through behavioural exposure, the (mistaken) beliefs which are considered to underlie and maintain his disorder.
CONCLUSION
Conceptually, this is an exciting time. Following their birth in the late 1950s behavioural techniques of anxiety reduction had their most rapid period of development during the 1960s and 1970s, by which time behavioural exposure had become the accepted treatment of choice for phobic anxiety disorders (Marks, 1978a, 1978b). While, in terms of technique development, the period since then may be regarded as one of relative stagnation, it may yet prove to be a significant time.
Progress in science normally comes through conceptual reformulations, or “paradigm shifts”. The problem in clinical psychology has been that most changes in theoretical positions have spawned a new set of therapy techniques, with a tendency simply to ignore the techniques associated with earlier theories. Thus it often appears as if each new formulation means beginning again – change with no clear sense of progress.
Perhaps with behavioural exposure treatment of panic disorder/agoraphobia we are at last seeing the possibility of conceptual change resulting not in the abandonment of a previous technique but in its improvement. The question is no longer about whether exposure works, but how it works (Bandura, 1977; Beck et al, 1985; Clark, 1986), and how it can be improved. The Cognitive Invalidation Model is offered as one contribution to this enquiry.
REFERENCES
Agras, S., Sylvester, D. and Oliveau, D. (1969) The epidemiology of common fears and phobias, Comprehensive Psychiatry, 10, 151.
Agras, W.S., Chapin, H.N. and Oliveau, D.C. (1972) The natural history of phobia: course and prognosis, Archives of General Psychiatry, 26, 315.
Baker, R. and McFadyen, M. (1985) Cognitive Invalidation and the enigma of exposure. In E. Karas (ed.), Current Issues in Clinical Psychology, Vol. 2, Plenum, New York.
Bandura, A. (1977) Self-efficacy: towards a unifying theory of behaviour change, Psychological Review, 84, 191.
Beck, A.T., Emery, G. and Greenberg, R.L. (1985) Anxiety Disorders and Phobias: A Cognitive Perspective, Basic Books, New York.
Buglass, D., Clarke, J., Henderson, A.S., Kreitman, N. and Presley, A.S. (1977) A study of agoraphobic housewives, Psychological Medicine, 7, 73 – 86.
Burns, L.E and Thorpe, G.L. (1977) Fears and clinical phobias: Epidemiological aspects and the national survey of agoraphobics, Journal of International Medical Research, 5 (Suppl. 1), 132-9.
Clark, D.M. (1986) A cognitive approach to panic, Behaviour Research and Therapy, 24, 461-70.
Epstein, S. (1972) The nature of anxiety with emphasis upon its relationship to expectancy. In C.D. Speilberger (ed.), Anxiety: Current Trends in Theory and Research, Vol. 2, Academic Press, New York.
Freedman, R.R., Ianni, P., Ettedgui, E. and Puthezhath, N. (1985) Ambulatory monitoring of panic disorder, Archives of General Psychiatry, 42, 244-8.
Goldstein, A.J. and Chambless, D.L. (1978) A reanalysis of agoraphobia, Behaviour Therapy, 9, 47-59.
Hallam, R.S. (1978) Agoraphobia: a critical review of the concept, British Journal of Psychiatry, 133, 314-19.
Hallam, R.S. (1985) Anxiety. Psychological Perspectives on Panic and Agoraphobia, Academic Press, London.
Kelly, G.A. (1955) The Psychology of Person Constructs, Vols 1 and 2, Norton, New York.
Kelly, G.A. (1963) A Theory of Personality, Norton, New York.
Kelly, G.A. (1970) Behaviour is an experiment. In D. Bannister (ed.) Perspectives in Personal Construct Theory, Academic Press, London.
Klein, D.F. (1964) Delineation of two drug-responsive anxiety syndromes, Psycho-pharmacologia, 5, 397-408.
Klein, D.F. (1981) Anxiety reconceptualised. In D.F. Klein and J.G. Rankin (eds) Anxiety: New Research and Changing Concepts, Raven Press, New York.
Klein, D.F., Rabkin, J.G. and Gorman, J.M. (1985) Etiological and pathophysiological inferences from the pharmacological treatment of anxiety. In A.H. Tuma and J.D Master (eds), Anxiety and the Anxiety Disorders, Lawrence Erlbaum, Hillsdale, New Jersey.
Lazarus, R.S. and Averill, J.R. (1972) Emotion and cognition: with special reference to anxiety. In C.D. Spielberger (ed.) Anxiety: Current Trends in Theory and Research, Vol. 2, Academic Press, New York.
Lazarus, R.S. and Launier, R. (1978) Stress-related transactions between person and environment. In L.A Pervin and M. Lewin (eds), Perspectives in International Psychology, Plenum, New York.
Marks, I.M. (1978a) Exposure treatments: clinical applications. In W.S. Agras (ed.), Behaviour Modification: Principles and Clinical Applications, 2nd Ed, Little, Brown and Co., Boston.
Marks, I.M. (1978b) Exposure treatments: conceptual issues. In W.S. Agras (ed.), Behaviour Modification: Principles and Clinical Applications, 2nd Ed, Little, Brown and Co., Boston.
Mathews, A.M., Gelder, M.G. and Johnson, D.W. (1981) Agoraphobia: Nature and Treatment, Guildford Press, New York.
Pitts, F.N. and McClure, J. (1967) Lactate metabolism in anxiety neurosis, New England Journal of Medicine, 277, 1329-36.
Sheehan, D.V. (1982) Panic attacks and phobias, New England Journal of Medicine, 307, 156-8.
Snaith, R.P. (1968) A clinical investigation of phobias, British Journal of Psychiatry, 114, 673.
Spielberger, C.D. (1966) theory and research on anxiety. In C.D. Spielberger (ed.) Anxiety and Behaviour, Academic Press, New York.
Stampler, F.M. (1982) Panic disorder: description, conceptualisation, and implications for treatment, Clinical Psychology Review, Vol. 2, 469-86.
Postscript, December 2020
The development of the Cognitive Invalidation Approach to Panic Disorders (and how it differs from Beck’s Cognitive Theory/Therapy)
While the chapter is a reasonable account of the approach at the time of publication, it is not a full account of how the approach developed, and what factors contributed to it. In order to answer the perennial question of how it differs from Beck’s Cognitive Theory/Therapy it may help if I describe how The Cognitive Invalidation Approach (CI) came about and where it is now.
I am frequently asked about the influence of George Kelly on my work. For those of us who reject the the behaviourist concept of man as the product of associations, reinforcements and punishments, and psychoanalytic man as the survivor of the battle between the unconscious id, ego and superego, Kelly offers”inquiring man”, man the (amateur) scientist, the I think therefore I am man, or as I prefer it, the I am therefore I think man. It is the nature of man to try to make sense of his experience, including environmental reinforcements and the unconscious. However it is not the event itself which determines behaviour but how we perceive the event. As usual a first century Greek philosopher, Epictetus, was way ahead of us with this one.
I would claim that there is evidence for Kelly’s inquiring man. In his epochal 1956 work, The Normal Child and some of his abnormalities, largely based on observational study and analysis, C W. Valentine makes the obvious case that from birth children actively interact with their environment for the purposes of learning and entertainment. How difficult it can be to see the obvious! Incidentally , he also made the case for the normality of many of the behaviours labelled as psychopathological by the psychiatry of the day. No change there (see “Saving Normal”, by Allen Frances, 2013).
Why is the approach called Cognitive Invalidation?
Validation and invalidation are both part of Kelly’s system, where validation occurs when the expected happens and invalidation when the expected does not happen. Invalidation is the more important because it promotes change.
Although I took much inspiration from Kelly in terms of the model of ‘inquiring man’, sense-making, the validation/invalidation process and what eventually became ‘behavioural experiments’, the CI Approach is not a part of Personal Construct Psychology.
Historically, I see CI as belonging with the series of exposure based therapies such as Systematic Desensisation, Prolonged Exposure, and Flooding. Deconditioning and habituation were seen as the processes whereby these therapies worked. For me CI provides a better explanation of the process of how Panic Disorder develops and how exposure based therapies work.
CI is essentially a self managed process. It is the patient who both directs the experiment and is the subject. Kelly suggests the analogy of the therapist as supervisor, who can provide information and advice which the patient can take or reject, but it is the patient who is ultimately and necessarily in charge.
While I continued to develop CI, by listening to patients describe their experiences with, and understanding of, their PD, the group of Gelder, Marks, Rachman et al, from whose work I took my inspiration, rather abruptly switched their attention to Beck’s Cognitive Theory/Therapy. This followed a period of close collaboration between Professor Aaron Beck at the University of Pennsylvania and Professor Michael Gelder at the University of Oxford. During the 70s there were frequent staff exchanges between the two universities and Oxford became an outpost and development centre for Beckian Cognitive Behavioural therapy. It will be clear from this website that I believe that the subsequent emphasis on Beckian Cognitive theory and therapy, and the relative neglect of the development of the behavioural and affective components of CBT has been a retrograde step with literally global consequences for PD sufferers.
I have addressed the logical and psychological flaws in Beck’s Cognitive Theory and Therapy in my paper (McFadyen, 2020) which opens this website.
The final part of the CI approach to be developed was the key to answering the question of how CI is different to Beck’s Cognitive Theory/Therapy. Listening to PD sufferers describe their experiences with panic attacks (PAs) it eventually became impossible to ignore the conclusion that panic attacks are NORMAL reactions to ABNORMAL circumstances. This was not so much a lightbulb moment as a gradual confirmation that this made the most sense of patients’ descriptions of their experiences (Baker and McFadyen, Cognitive Invalidation and the Enigma of Exposure, in Karas Ed., Current Issues in Clinical Psychology 2, Plenum 1985).
Not only can we almost always identify stressful life circumstances as a forerunner of PD but we can identify environmental factors affecting specific groups of sufferers.
One clear group was bank staff during the period when banks were pressuring customer-facing staff with increasing targets to sell insurance and investment products (which mostly turned out to be totally unsuitable, requiring the banks to later reimburse customers). Another group was of school classroom assistants who were being pressured to undergo teacher training courses when the Scottish Government was desperately trying to meet electoral promises of increased staffing. And of course NHS staff who were constantly being reorganised.
A particularly interesting group was the farming community when farming became subject to the Common Agricultural Policy and subsidies which led to food ‘mountains’ and other problems. The younger generation who had to accept CAP directives in order to keep farms solvent found itself in conflict with the older generation. Older farmers presented with depression from loss of purpose while younger farmers presented with anxiety/panic disorders.
Therapy associated with the CI approach
Within CI panic attacks are seen as being a normal response to these life stresses, but understandably sufferers cannot readily make sense of it all. However it is not ‘catastrophising’ to think that panic attacks are dangerous. We only know this through experience, either direct personal experience or information from trusted sources. As we shall see, both of these are central to the CI approach to panic disorders. There is usually no need to provide separate Cognitive Therapy as behavioural experiments naturally change cognitions.
Therapy associated with the Cognitive Approach
Within Cognitive Therapy as per Beck and Clark, sufferers are first told that their PD is caused by their faulty, irrational, thinking. They are then subjected to various educational techniques to restore their thinking to ‘normality’. Initially time is spent on eliciting automatic thoughts and dysfunctional assumptions, using “the art of Socratic questioning”. In addition to these more directly cognitive techniques patients may be given a variety of other skill training activities such as breathing training, in-office attempts to elicit PAs etc. Some therapists recommend asking the patient to hyperventilate to attempt to bring on a panic attack (I don’t recommend this as I do not consider it an appropriate analogue experience and it is not free of risk). One of these techniques is behavioural experiments very similar to CI behavioural experiments although in Cognitive Therapy it is usually considered as secondary to the more direct ‘cognitive’ techniques, the idea being that the cognitive therapy prepares sufferers to make more veridical interpretations of PAs.
Within the CI approach sense making and behavioural experiments are the core techniques.
CI Approach: Typical first session
There are generally only three stages in the therapy associated with the CI approach. I prefer all three stages to be completed at the first session since this allows the patient to leave with the confidence that, 1 they are normal and 2, they can overcome PD.
The first stage is much the same as in all psychological therapy. I ask open questions to encourage the patient to tell their story in whatever way they choose. I answer any questions they ask, and may ask them questions to get a fuller picture of the problem they present.
If the problem is PD I will ask what they know or have been told by others about PD or PAs.
In the second stage we talk about how PAs occur and how PD develops. I start with a single A4 blank sheet of paper. On it I will show them how our base arousal level changes with demand – low when we are relaxed and inactive – higher when we are, for example, driving in busy traffic.
I continue with something like,“Let’s say that while we are driving along a car pulls out of a side street in front of us and we have to make an emergency stop. The base system is too slow to help us respond but fortunately we have a second emergency system which ‘kicks in’ and with luck we narrowly avoid an accident. Some friend plays a prank and gives us a fright by jumping out from a dark doorway. The same system comes into play making our heart beat much faster than normal, our breathing increases, and our muscles tense in readiness for action (sometimes referred to as the fight or flight response), but very quickly we know the situation is not dangerous and the reactions subside”.
{I prefer not to use terms like autonomic nervous system or neurochemical transmitters. In my experience these are unnecessary distractions. The simple drawings on the sheet of paper are not physiology notes but a heuristic which patients relate well to, despite it consisting of a few straight lines and some squiggles}.
We discuss the differences between these two situations and a panic attack. In terms of how we feel everyone agrees it is not very different, except that we know what has caused the first two situations. With a panic attack we do not know what is happening and that makes all the difference. I have never heard anyone say, “I had no idea what was happening to me so I did not get concerned”, or, “so I just ignored it”. Now those would be abnormal reactions! I may share this observation with the patient
I show them that when we are significantly stressed our base arousal system moves to a higher level – we feel more on edge, more ready to react. At these times our emergency system is also more ready to react, and like any other emergency system, it occasionally triggers a false alarm. The false alarm emergency reaction usually triggers a real emergency reaction making the situation frightening for the reason we have already talked about – that we don’t know what is happening, but whatever it is it is pretty scary.We then talk about what they fear might be happening and this gives the usual responses of heart attack, unable to breathe, going to die, feeling in danger of passing out, making a fool of myself, losing control, often undefined. Throughout the session I acknowledge the normality of their fears.
Finally we talk about what they need to do to prove to themselves that PAs are not dangerous. Their answer forms the basis of therapy. For some patients the first session is all that is required. They have their behavioural experiment plan and it works. Others will take longer to complete a more multi-part plan. They take the sheet of paper home and can help themselves to a patient leaflet. Based on my colleagues and I the average in-office time is around 3 and ½ hours, beginning to end.
Beck’s observations
In his paper Cognitive approaches to Panic Disorder: theory and therapy (Beck, A T, 1988, in Panic: Psychological Perspectives (eds Rachman S and Maser JD, p91) Beck has this to say about the Cognitive Model. “The Cognitive Model of panic disorders is essentially a descriptive model. It is derived from clinical examination ……..In a previous description of panic attacks I pointed out the following characteristics of the patient’s fear during the attacks……….From the patient’s standpoint the danger is quite real and plausible……….Often but not always the acutely anxious patient is overwhelmed by thoughts that he is dying”.
In the same piece he describes such thoughts as “panicogenic”. By this he means that PD patients have a predisposition to be “particularly sensitive to internal sensations (somatic or mental) that do not seem normal”. He adds that crucial to the experience of panic as contrasted with simply severe anxiety is a final stage where the patient loses the capacity to appraise the symptoms realistically. At this point the patient is “scared out of his wits”.
Beck’s observations of the fears of PD patients are well known, which suggests to me that they are the common responses to PA. Pitts and McLure while researching the effect of sodium lactose infusion in anxiety disorders quote an interesting remark by a ‘normal’ control subject who said,” If I didn’t know you were doing this to me and that you wouldn’t let anything bad happen to me I would be certain I was dying of a heart attack or something terrible”. There would have to be very strong evidence to counter the most obvious interpretation that these responses are the normal reactions of normal people to the normal experience of a PA. There is no need to postulate that the thoughts are ‘panicogenic’.
It is unfortunate that in the merger of behaviour therapy and cognitive therapy to form CBT, Beck’s Cognitive Theory and Beck’s Cognitive Therapy became the dominant influences. Once it is recognised that PAs/PDs are essentially normal reactions to abnormal circumstances/events rather than being caused by the faulty thinking processes of the sufferer, we have a normal, natural process in Cognitive Invalidation to allow PD sufferers to make sense of their experience through more appropriate information and self-directed behavioural experiments.
Back to the question of what is the difference between CI theory and therapy and Beck’s Cognitive theory and therapy?
In terms of theory the CI approach to Panic Disorders does not require us to postulate any cognitive predisposition in the sufferer, or any cognitive distortions, or indeed any other cognitive abnormality. What is wrong with the sufferer is that he very normally and reasonably misinterprets his panic attack as dangerous in some way (physical, e g heart attack; mental, losing my mind; or social, making a fool of myself) – just like any other normal person.
In terms of therapy, the provision of ‘sense-making’ information and the opportunity to confirm for himself, through behavioural experiment, that PAs are not dangerous is it. Two short ‘stories’ will illustrate the therapy.
The first is a lady in her 50s who presented with a 20 year history of agoraphobia and who could not remember when she last left the house on her own. The very thought of doing so often resulted in a panic attack. The panics had started when she was caring for her dying mother. The reason for presenting was that she wished to fly to see her son who lives in the USA. In the session, when we went over what she knew about PAs, she was somewhat embarrassed to admit that she knew virtually nothing. She had not been given any information by her GP other than the diagnosis of agoraphobia. Since she never went out unaccompanied by her daughter she had stopped taking medication many years previously. She was surprised that she had not been given the information when she initially saw her doctor, but accepted that things were less well known then. Her main fear was that she would collapse “or worse”. When asked what she needed to do to convince herself that panic attacks were not dangerous, she immediately said she would have to go into the town, which she duly did within the week, tolerating quite a few PAs particularly at the check outs. Some weeks later she returned to report that going into town was no longer a problem, and that whatever she did in town, including shopping, she could not bring on a panic attack. She thanked me profusely telling me that the explanation of her PAs had been what helped her most. Some months later she returned to tell me she had had a great holiday with her son and family. In the week after she had arrived her son had arranged to take her to an ‘Aggies group’, thinking it might help her. When she told them how she had overcome her fear, someone had arranged for her to go on local community radio where she had been a big hit. Since she had returned home she had heard from two people who had similarly overcome their fears inspired by her personal account. Effectively this was a one session ‘recovery’ after 20 years of suffering PD. I would not consider her in any way typical. But it demonstrates the power of (the right) information – information which makes sense to the patients – information which enables them to risk the consequences of a panic attack.
The next story concerns a 20 something nurse who asked for help because it was coming up to Christmas when each year, she would feel “panicky” at the prospect of having to help decorate the ward, which involved balloons. From a child she had been “phobic” about balloons. She could not remember how it started but her mother had told her that she used to “scream the place down” whenever balloons were around at family birthdays or whatever. She assumed that this was when balloons burst, and anticipation of this was still a main part of her fear. Eventually all the relatives would avoid having balloons at family parties. Since then she became anxious even seeing balloons in a shop window and would go out of her way to avoid balloons. But the main problem was the constant anxiety every year in the months before Christmas. At work she was having to make excuses why she did not join in decorating the ward, or suffer extreme anxiety when she had to be involved, which was usually for as short a time as possible. She had been considering changing her job which she very much enjoyed, when she decided she had to try to do something about her problem before doing that. At our first session she was quick to say she could understand how it had come about, with the over-concern of family having prevented her from contact with balloons “until it was too late”. She had a “good idea what was likely to be involved”, but was afraid she might make matters worse trying on her own. When asked what she thought she needed to do she said she had read about desensitisation and flooding and thought some sort of flooding might be best but was not sure how it would go. I asked how she could find out how it would go to which she answered “I’ll just need to try it and see”. We agreed she had a good plan for her behavioural experiment and discussed practical details like where and when, given there would be some noise. With that sorted she volunteered to find a friend who would burst balloons when she had her eyes closed and when she had her eyes open. She might burst some balloons herself to “get the feel of it”. She and her friend obtained balloons and balloon nets etc. and over a week period they had three 15 minute sessions. She was very anxious just getting the balloons and accessories, and when her friend burst balloons in the session. By the end of the first behavioural experiment session she described herself as “shattered” but exhilarated at having “survived” the anxiety feelings. In the second session she instructed her friend to drop a netful of balloons on her, which she and her friend burst in many different ways. Again she reacted with significant anxiety but “felt great” afterwards. The third session was like the second session but on her own. She acknowledged some twinges of anxiety but a great sense of achievement. After the Christmas holidays she reported having had the best Christmas at work ever and added that she also had learned a lot more about psychological therapy than she had got from any book. So had I, and I felt good about the outcome too. This was a fairly simple case which exemplifies the process, and advantages, of collaborating on both formulation and behavioural experimentation.
